Enlightened Practice Podcast
Our hosts, Dr. Ken Braslow and Dr. Kari Kagan, share some reasons why to switch from a current EMR/EHR to a new service, how much time it may take, the features to consider when making the switch, and the impact on patients and clients. Invite your colleagues to tune in and learn more about the most user-friendly, affordable EMR/EHR for mental health practitioners, Luminello.
If you want your question featured and discussed on the show, send it to [email protected]. We’d love to hear from you.



Transcript of the podcast
Ken: Hi Kari. Welcome back to the podcast.
Kari: Hi Ken. Thanks for having me.
Ken: Sure. Happy New Year!
Kari: Happy New Year to you too.
Ken: So, we’re going to start off the New Year by talking about change and growth in your administrative life. Not the most exciting topic potentially, but today, I was thinking we could be talking about the process of switching electronic health records and what to do if you find yourself with a vendor who you don’t want to continue with for whatever reason. And the challenges in switching over to a new EHR, and the logistical challenges, psychological challenges, time challenges, and how to think that through so, our listeners can decide if that’s a decision they want to go through with. First, let’s start off, have you ever switched EHRs?
Kari: Yes, I have switched EHRs, and I will be the first to say that it definitely is a process. It can be a big undertaking just depending on the size of your practice, how many years you’re going to practice, but I could say without a doubt it’s worth it if it’s going to increase the efficiency of your practice and your business. So, it’s definitely a short term pain for long term gain experience and it is important to maintain that long term perspective if you do decide to switch because it will definitely make your life easier in the long run, but it can be giving more time and energy in the short run to make it happen.
Ken: Yeah, I wish there was a switch that could reflect and data could seamlessly go through the invisible ether and come into another platform. We’d love to have that so people could switch to us easily, but we get that it’s a process and that it takes a lot of planning and thoughtfulness to it. So, I thought we’d go through today some of the pros and cons of the various aspects of it. I was thinking that there’s multiple things that you should be looking for broadly in an EMR or an EHR, one of them would be functionality, of course, does it do what you need it to do. Not just basic functionality but how are the workflows designed? Do they anticipate how you think about the administrative needs as your practice?
So that way when you get up and running with a system it doesn’t drain you of energy. You know, if you have workflows that are not intuitive than it hurts your brain. You have to Google the answer or go look in the support site, or just click around a lot and that’s pretty painful. I think when any clinician is evaluating any EHR/ EMR to begin with or to switch to, thinking about not just how powerful it is, but how graceful that power is, how efficient it is, how few clicks you can accomplish or task it is really meaningful.
Kari: Right.
Ken: So, I’m curious, when you were switching your EHR, what were you thinking about, what drew you to your new EHR?
Kari: Yeah. I was thinking about what would work for my practice, like really similar to what you’re describing. I wanted something that was efficient, easy, as effortless as possible because at the core of what I do, I’m a clinical psychologist and I want to be able to spend my time focused on that not on the admin side of things. So those were my priorities, just something that could make the admin side of things as simple and easy as possible. And then also, I was looking for ease in terms of the transition. A lot of EHRs have the support to help make the transition because many people do transfer.
So, again that was something. Again, it goes under the same umbrella, like make everything as easy as possible including the transfer itself. So, I was looking for support features and making the transition. I think you summarized it well when you said intuitive. It didn’t require looking up a lot of frequently asked questions to figure out how to do some basic stuff like scheduling or creating a note, or something like that.
Ken: Yeah, makes sense. I think going along with that is if you do have questions, having really top notch customer support, hopefully they never need to answer anything. Kind of like the repair man who is always sitting around, has nothing to fix, so he’s pretty bored, that’s the ideal, but inevitably questions come up and feeling like you can ask a question and it doesn’t just go into the ether and it takes a year and half to hear back.
Kari: Right.
Ken: You want fast response time, but you also want well trained customer service. The challenge with customer service is those folks are not clinicians. They know the software or they can run the software, but they don’t know how clinicians like us think. So, the amount of training that a customer service team gets into how clinicians think is pretty evident in when you get started because you’ll get two different kinds of answers. If they’re just well trained in the software, you’ll get basic answers of how to do things. But, if they’re well trained in how clinicians think, you’ll get answers about what makes more sense for you and your practice, about how to use that feature.
Kari: Yeah.
Ken: The other thing is that some folks like more official training. They don’t want to learn everything new on their own. So, what we find is that there’s two different segments of clinicians. One, they just don’t even talk to them. They’ll just click around and figure it out. And then, others who want webinars and they want kind of custom one-on-one training experience. So, that’s something that’s worthwhile that you should be looking for as you think about how you are going to wrap your mind around this new endeavor. I’ll just add one point. It’s not just about you. It’s also about if you’re in a group of clinicians, how easy it is for the biller to learn it. Is there training for the biller and the scheduler? And also for your clients and your patients, what is their experience like? Because EHR is an extension of your practice, that’s where they’ll be presumably logging into pay their bills or book appointments and things like that. And if the experience is intuitive and graceful for them that can only serve to help your practice. And if it’s painful for them and they run into bugs, you’re going to hear about it and that gets you off your game.
Kari: Right. Those are all good points.
Ken: So, let’s talk a little bit about, how much did you spend in transitioning and how did you think about getting your information over from your old system to your new system?
Kari: It is quite an investment of time to do this. I mean, you can take it in chunks or you can do it all at once to make it feel more manageable for you. I kind of did a combination when I personally made the transfer. So, just because I was actually curious to learn the new system and the EHR, I initially took a chunk of time out of a day to personally create some of the charts and play around with some of the note templates and stuff like that. I had to customize it the way I wanted it and I did several charts in a row basically for myself to invest the time to getting the practice to eventually get to that point where it felt more effortless and efficient to make it as efficient as possible.
So, I did that initially when I was making the transfer, but then especially if you’re seeing a lot of clients it can take quite a lot of time to do that. I just kind of did it as I set up charts and customized things the way I wanted to as I went after I saw different clients. And that felt more manageable for me just to take it slow and there really isn’t a huge urgency to get everyone in at once. You really can just go client by client as you see them. And I think is also helpful to inquire as to whether or not EHR has the customer support to assist with the transfer, if they can also do things to make it easier to transfer, like charts for you and input different data points from your previous chart into it. So, that’s something to make sure you look into before you decide to make the switch because that can make it go much smoother and quicker.
Ken: That makes sense. Of course, I’m biased in talking about switching EMRs since I founded Luminello, but I will say that I myself had to switch EMRs from my previous EMR to Luminello, as customer number one. The previous EMR I was using did not make it easy for me because they really had no incentive to and I used the process of me switching over to start to inform how we could make the process go better for other clinicians switching over. My experience was that I did end up keeping my old EHR subscription for a couple of months, just because I didn’t want the pressure of having to do everything in one marathon weekend.
Although, we do have some users who tell us they do just spend a whole weekend or take a day off from work and they’re done. I didn’t want to go that route. So, like you, I invested more time in the beginning in making sure that it actually met the standards that I needed for my own clinical practice. Then, over time as I saw the patients normally in the course of my practice, at the beginning of the day I would make sure that their charts were set up and ready to go. And what I ended up doing was I would have my old system open and Luminello open and I would just copy my most recent note from my old system and it became the first note in Luminello. So at least I had that.
And then, when I had more time I would download a PDF of the old chart and upload a PDF into the current chart. So, it wasn’t painful but it wasn’t instant. You couldn’t just snap your fingers and make all the data appear. But it worked pretty well and I used it as an opportunity in sessions. I would say to patients, I’m switching systems and I just want to make sure I have all your correct info. And actually there were a bunch of people who had moved and I didn’t even know. It was a good opportunity to make sure all of their demographic info, all of their insurance info was actually correct. It’s probably something I should be doing more anyway.
So, I kind of folded those into the process. I had patients go in and update their own info sometimes if we were running out of time in session and I didn’t want to burn the time in session to do it. But mostly, it wasn’t the most painful process in the world because I set myself up to not get overwhelmed with it and I think that’s really important. It’s a nice feeling to have everything neat and tidy and wrapped up in a day, but it’s maybe not realistic for most people and if you put yourself under that pressure then it’s not going to feel good inside. You should go at the rate that feels right for you, but it’s fine for it to be a process and for it to take some time. That helped me relieve my anxiety about switching from my old system.
Kari: Yeah. And I agree too on the point that it was actually a good opportunity to just refresh charts and to make sure all the information was correct and even sometimes to review old notes and it actually was like a professional development experience too from a clinical perspective. So, while there are challenges, I think the benefits in terms of just checking in on each client and in that kind of way that we don’t usually do necessarily. But also, the long term benefit of hopefully having a charting system that works much better for you.
Ken: What did you do with the charts for clients you weren’t seeing any longer?
Kari: Yeah, that’s a really good question. So, what I personally did is keep them in the former EHR that I was using and the system that I was using before allowed for that. So, I could just keep my log in information and as a psychologist you have to maintain records for 70 years after you’ve stopped seeing someone. So, for anyone that I had stopped seeing, if for some reason I needed access to their records, I could just log into my old EHR system, but I know that someone might not be able to do that.
I think this would be a good thing to discuss with a potential new EHR you’re switching to, but I’m pretty sure a possible solution for that is to download a PDF of the whole chart and save it either in the new EHR or even in a HIPPA compliant folder so you have access to it is because it is important to hold onto old records, whatever is required of your profession and I think that’s actually pretty easy to do just downloading a PDF.
Ken: Yeah. I’d say, you really have to think about what function does it serve to transfer over old charts other than for regulatory reasons? If you’re really not actively working with them it’s going to make the process much smoother if you break it down into current charts and old charts. I think it will be a lot less overwhelming to just focus on current charts. So, just to touch on the HIPPA compliant part of what you said because I think it’s really important, if you’re going to download PDFs from your old EHR, you can just store them on your hard drive, that would be the simplest. But you’ve got to make sure that your hard drive is encrypted. And with Max, they call it volte volt and you want to make sure that’s turned on and the newest edition of Windows has hard drive encryption standard, older versions of Windows do not.
And you may need to upgrade to a more recent Windows operating system that does have it. And then what if your hard drive crashes? Now you’ve got a dilemma. So, you should be backing up that hard drive and the same caveats apply that your hard drive backup should be encrypted. That means, if somebody steals your laptop or your hard drive, if it’s encrypted you have a pretty strong defense against any HIPPA claims because HIPPA is not assuming that nothing bad ever happens, they get that there’s badness in the world.
But, you have to take reasonable measures to protect against it. And by not just having a password on your hard drive, that’s a really important part but a password has nothing to do with encryption. Because, if somebody stole your laptop and it was just password protected, they’d just take your hard drive out and hook it up to their laptop and then they could see everything. So, as long hard your hard is encrypted and password protected ten you have really strong grounds, but you’re also doing the right thing by protecting your client’s stuff.
If you’re going to store your charts in the cloud, then you better have a business associated agreement signed if you’re going to do it with Google or Dropbox. And that doesn’t just mean like saying, yes, they’re HIPPA compliant. You need it in writing and they will send you a signed BAA to print, you’ll need that and you’ll need to store that in a safe place so that way if anything ever happens, again, you showed that you did your due diligence. That’s really meaningful.
When you break down your system into current charts and old charts, it just really reduces the cognitive burden on your brain because then, okay now, you have the current charts and if you’re going to do the easy as you go up approach and you’re seeing five or eight clients a day, then slowly over time you will get there and it doesn’t seem as overwhelming. But if you have thousands of old charts you’re going to feel it even before you began, but it’s reasonable.
Kari: Yeah.
Ken: If an old client comes back to your practice, you can always as a one-off create a new chart for them in the new system and then go find that old chart wherever you stored it and upload it.
Kari: Yeah.
Ken: So, few other things to think about are billing, calendar, we talked a little bit about copying notes in. But, for billing, most systems will allow you to have an initial balance. What I did with my old EHR was I sent them a lifetime statement and that way they had it for their records, because you know, if you switch in January and people come to you in December saying, oh, I need a statement for my records. That might be challenging for taxes for the following year. So I sent them a lifetime statement. So it was covered.
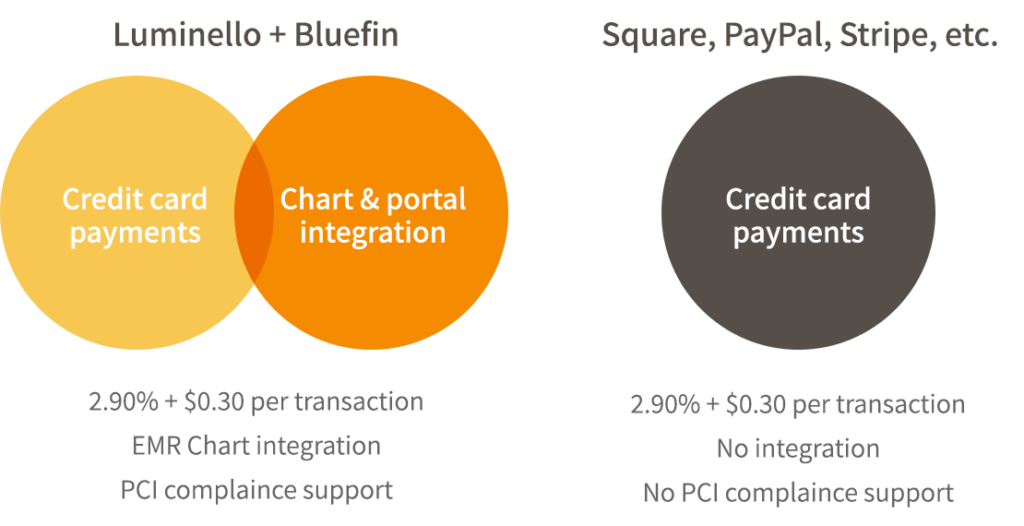
And then I just told them, we’re moving onto a new system and can you please enter your credit card info, next time you log on. It’s really, really meaningful to have the patient or client enter their credit card info because then your requirements for PCI compliance plummet and you have to do very, very little.
If you enter a patient or client credit card info then conversely your requirements for safely handling that info sky rocket. So, we highly encourage clinicians as part of their practice policies to never enter a patient credit card. And then, your PCI compliance annually is like a minute. It’s like 10-20 questions, check, check and you’re done. That’s one way to make it simpler. I’m curious do you remember what you did for your billing?
Kari: It’s a good question and it was a long time ago, so I can’t say that I totally remember. But my digging really deep into my memory is that yeah, I just asked all my clients to enter their credit card. I can’t entirely remember but I’m pretty sure I just asked them to enter their credit card information. I don’t remember sending one final statement from the previous chart before switching to the new chart. I really can’t remember, somehow, it worked out. It was a smooth transition and once the new billing was up and the credit card was up in the new chart, then I just started sending super bills from that place and it worked out. So, I think it really was as simple as telling your client to go into their chart and put a credit card in and that was it.
Ken: Great. What about your calendar?
Kari: That’s a good one. I also think what I did and again this was a really long time ago so it’s hard for me to remember, but I just had both the charts open and I personally just went in and created new appointments in the calendar. I didn’t have it imported. I’m not sure how that works. You would know better than me. I have a smaller practice so it doesn’t take as much time and I tend to be kind of controlling when it comes to my chart. So, I think, I just went in and literally put each appointment in the calendar and clicked repeat if it’s a repeat appointment, and all that kind of stuff. And also that way, I could make sure that everything was up to date because sometimes I would have old appointments that needed to be changed to bi-weekly but I hadn’t done it yet and I was just doing it as I went. So, it was just another one of those opportunities where I was like, okay, I can really clean up here. So that’s how I did the calendar.
Ken: Yeah, that sounds similar to my experience. And again, I used it as an opportunity to re-access my schedule and I ended up making some changes in the schedule.
Kari: Yeah.
Ken: As I was recreating appointments realizing, oh, why am I seeing this person at this time? I used it to clean things up a little bit. Yeah, it’s not like I see a thousand patients per week, so it didn’t actually take that long to set it up. And it’s not like you need to set things up for ten years out. You could at least set up amongst work appointments that probably wouldn’t take too long. It does take a little bit of time. There’s no instant calendar creation. I created the first month’s appointments in the first go-around because let’s say half of them were recurring but it went much faster for months two and on. This might be where you could also think about will your new EHR/ EMR assist you with this process and do you want them to assist you? Do you want the control over it? But again, breaking things down into smaller chunks so that way it’s not overwhelming.
Kari: Yeah, exactly.
Ken: So, any other thoughts that you have or advice that you might give about the switching process and the pain points?
Kari: Yeah. I mean, my thoughts are to really do your research and take your time figuring out what the best EHR for you is and if you really find one that you think is going to significantly improve the flow of your practice, it’s without a doubt hundred percent worth it. And just making sure it’s what you want, to the best that you can before really using it, that it is really what you want for your practice. I would definitely recommend going for it because it’s something that you use every day, potentially for many, many, many years to come. So it’s totally worth it.
Ken: That’s interesting when you think about the different tabs you might have open in your browser and how many of them do you keep open all day, every day.
Kari: Yeah.
Ken: Your EHR is like your companion. Those are good points. Well, I appreciate your thoughts Kari on this process and invite our listeners if they have questions or have other strategies that they found were useful for them, to let us know and we’ll put it up on the website, and talk about it in our future conversations.
Kari: Sounds good.
Ken: All right. Thanks Kari. Look forward to chatting again soon.
Kari: Thanks, same here. Bye.
Ken: Bye.